Evidence-Based Cancer Options Beyond Surgery, Chemotherapy, and Radiation: What the Data Shows (2026)
Cancer remains one of the leading causes of death globally, but modern medicine offers a growing spectrum of interventions beyond the traditional “big three”: surgery, chemotherapy, and radiation. For patients seeking alternatives due to personal preference, comorbidities, or prior treatment experience, understanding which evidence-based strategies can support survival and quality of life is critical.
This article examines the highest-quality data on non-surgical, non-chemotherapy, and non-radiation approaches, including precision and immune-based therapies, clinical trial options, and integrative strategies. We emphasize realistic expectations, differentiating interventions that can control disease versus those that are primarily supportive.
1. The Reality Check: Why Evidence Matters
Multiple large studies, including analyses from Yale University and national cancer databases, consistently demonstrate that patients who refuse standard treatments in favor of alternative therapies alone experience 2–6 times higher risk of death within five years, depending on cancer type and stage (Cancer Research UK, 2024; Yale Medicine, 2023).
Key Takeaways:
No non-conventional therapy has been shown to reliably cure most cancers as a standalone treatment.
Cancer outcomes depend heavily on tumor type, stage, molecular profile, and patient-specific factors.
Delaying or refusing evidence-based therapies significantly reduces survival chances.
This reality underpins the importance of selecting interventions with the strongest data, even when avoiding surgery, chemotherapy, or radiation.
2. Evidence-Based Medical Therapies Outside Surgery, Chemo, or Radiation
For many cancers, there exist therapies that do not fall into the excluded categories but have proven disease-control potential. These include:
2.1 Immunotherapy
Immunotherapy leverages the body’s immune system to recognize and attack cancer cells. Common modalities include:
Checkpoint inhibitors: Drugs like pembrolizumab or nivolumab block proteins that inhibit immune responses. Highly effective in melanoma, non-small cell lung cancer, Hodgkin lymphoma, and certain solid tumors (Cancer.gov, 2024).
Cell-based therapies:
CAR-T therapy (chimeric antigen receptor T-cells) targets blood cancers such as leukemia and lymphoma.
TIL therapy (tumor-infiltrating lymphocytes) can induce remission in selected solid tumors.
Evidence: Some patients achieve long-term remission without chemotherapy or radiation, although eligibility depends on tumor type and prior treatments.
2.2 Targeted Therapy / Precision Medicine
Precision oncology focuses on drugs that specifically target genetic mutations or proteins driving cancer growth.
Examples:
Imatinib for chronic myeloid leukemia (CML).
Trastuzumab for HER2-positive breast cancer.
NTRK inhibitors for tumors with NTRK fusions (tissue-agnostic).
Clinical impact: For tumors with actionable mutations, these therapies can dramatically improve survival, often with fewer systemic side effects than chemotherapy (Mayo Clinic, 2023).
2.3 Hormone (Endocrine) Therapy
Certain cancers rely on hormones to grow. Endocrine therapy blocks these signals:
Breast cancer: Tamoxifen or aromatase inhibitors.
Prostate cancer: Androgen deprivation therapy.
These are particularly effective in hormone-driven tumors and are generally administered orally (Cancer.gov).
2.4 Active Surveillance / Watchful Waiting
For very slow-growing cancers, such as certain low-risk prostate or thyroid cancers, active monitoring may be appropriate. Benefits include:
Avoiding immediate invasive therapy.
Regular imaging and bloodwork allow for timely intervention if progression occurs.
Evidence: Randomized studies show comparable long-term survival in select low-risk populations (Rush.edu, 2022).
3. Clinical Trials for Novel Non-Traditional Therapies
For patients ineligible for or uninterested in standard therapies, clinical trials offer access to emerging interventions:
Immunotherapies and bispecific antibodies: Expanding beyond conventional checkpoint inhibitors.
Personalized cancer vaccines: Stimulate immune recognition of tumor-specific antigens.
Metabolic or repurposed-drug strategies: For example, metformin or ketogenic diet adjuncts may slow tumor growth in early-phase trials, but remain non-curative alone (Liv Hospital International, 2024).
Photodynamic therapy and hyperthermia: Heat or light-based modalities for accessible tumors.
Actionable step: Patients can search ClinicalTrials.gov using filters for immunotherapy, targeted therapy, or their specific cancer type to identify rigorously monitored studies.
4. Integrative and Supportive Strategies to Improve Quality of Life
These interventions do not treat cancer directly but are backed by randomized trials for symptom management and overall well-being:
4.1 Exercise
150+ minutes of moderate activity per week can reduce fatigue and may improve overall survival in some cancers.
Programs should be tailored to patient capacity.
4.2 Mind-Body Therapies
Yoga, meditation, cognitive behavioral therapy, and acupuncture reduce anxiety, depression, and pain.
Evidence supports improved psychological resilience during treatment.
4.3 Nutrition Counseling
Focus on maintaining healthy weight and balanced diets (e.g., Mediterranean or plant-rich patterns).
Supports treatment tolerance and overall health, though no diet alone cures cancer.
Key caution: Avoid unproven supplements or “natural cures,” as they may interfere with other therapies.
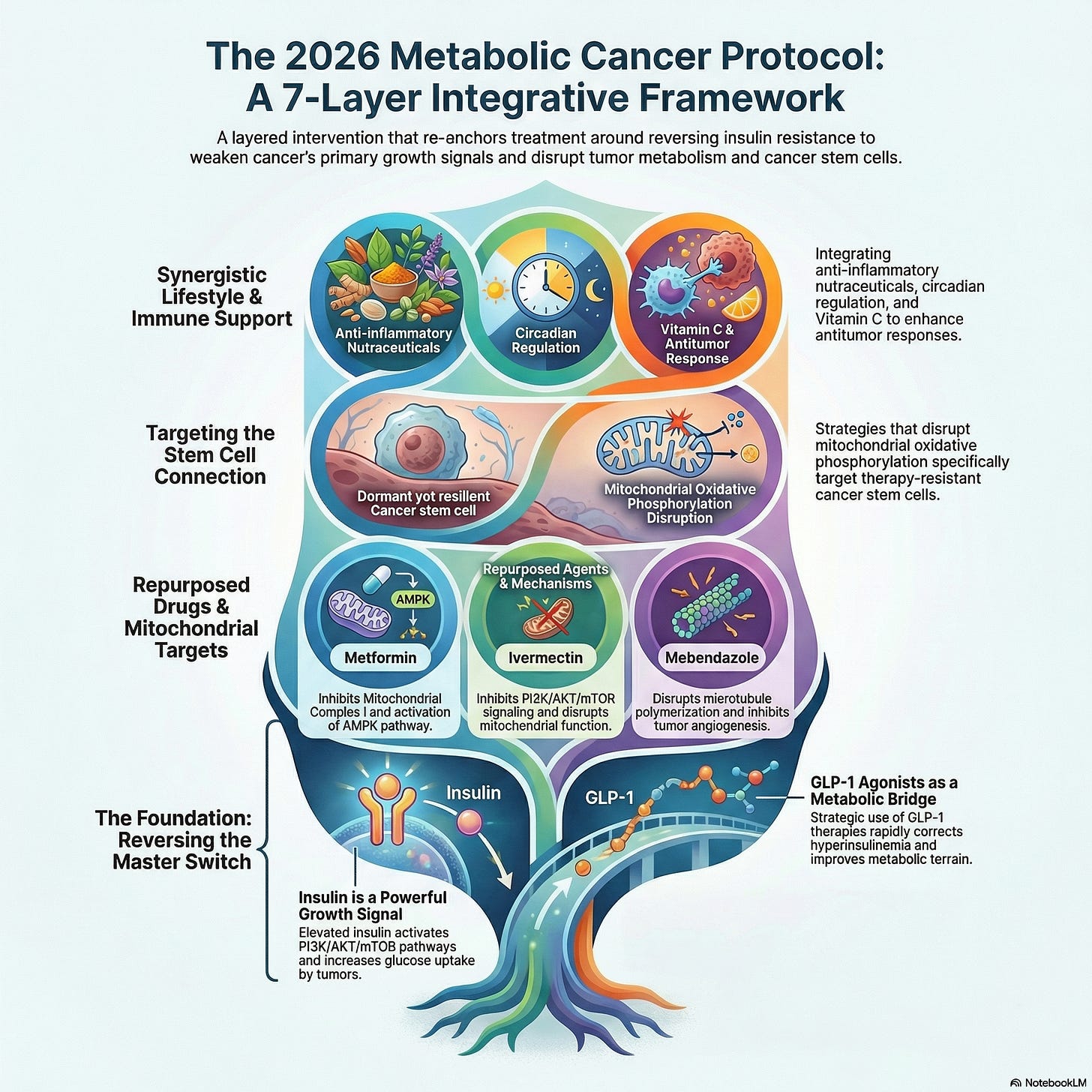
Read More: The Metabolic Cancer Protocol 2026: A 7-Layer Evidence-Based Strategy Integrating Metabolism, Immunity, and Precision Oncology5. Supportive / Palliative Care
Regardless of treatment choice, specialized supportive care improves both quality and duration of life:
Pain management, symptom control, and psychological support.
Nutritional interventions to prevent cachexia.
Early palliative involvement is associated with better patient satisfaction and improved outcomes.
6. Lifestyle Factors as a Foundational Layer
Even without surgery, chemo, or radiation, lifestyle interventions impact survival and recurrence risk:
Quit smoking and limit alcohol.
Maintain a healthy weight and stay physically active.
Consume nutrient-dense foods and reduce processed foods.
These are well-supported by cohort studies and meta-analyses as foundational cancer risk modifiers.
7. Critical Takeaways
Refusing standard treatments carries significant risk. Evidence consistently shows worse survival for patients relying solely on unproven alternatives.
Non-surgical, non-chemo, non-radiation therapies exist but must be selected based on cancer type, stage, and molecular profile.
Clinical trials provide access to cutting-edge therapies with careful monitoring, often years before standard approval.
Integrative strategies improve quality of life, but are adjuncts, not substitutes.
Lifestyle and monitoring are essential: quitting tobacco, exercising, nutrition, and regular imaging remain non-negotiable for best outcomes.
8. Next Steps for Patients
Obtain a detailed diagnosis: cancer type, stage, molecular profile, and actionable biomarkers.
Consult an oncologist or specialized center: NCI-designated or major academic hospitals often provide second or third opinions at low/no cost.
Explore precision and immunotherapy options based on molecular profiling.
Review ongoing clinical trials via ClinicalTrials.gov.
Integrate supportive care strategies early to maintain physical and psychological well-being.
9. References
✅ Conclusion
While no alternative therapy alone reliably cures cancer, modern medicine provides a spectrum of evidence-based, non-surgical, non-chemotherapy, non-radiation strategies. Precision oncology, immunotherapy, and clinical trial participation can offer disease control and even long-term remission in select cases, while integrative and lifestyle measures improve quality of life.
For patients seeking these pathways, the combination of informed clinical decision-making, supportive care, and active monitoring offers the best chance for meaningful, high-quality survival.

.png)




.png)



Comments
Post a Comment