Modified Citrus Pectin (MCP): The Anti-Metastatic Supplement? Evidence, Benefits and Research - Dr Paul Marik
Last updated: July 2026
Introduction
Modified citrus pectin (MCP) is a low-molecular-weight form of citrus pectin designed for absorption. It has attracted attention because laboratory research suggests it may bind galectin-3, a protein involved in inflammation, fibrosis, immune regulation and cancer metastasis. Although preclinical evidence is encouraging, human clinical evidence remains limited and MCP should not be considered a proven cancer treatment.
What is Modified Citrus Pectin?
MCP is produced by altering natural citrus pectin into smaller fragments that are more readily absorbed than ordinary dietary pectin.
Galectin-3 and Cancer
Galectin‑3 is a β‑galactoside–binding lectin implicated in tumor cell aggregation, adhesion, angiogenesis, apoptosis resistance, immune evasion, and organ fibrosis.(2)- Cell adhesion
- Tumor invasion
- Metastasis
- Angiogenesis
- Immune evasion
How MCP May Work
- May interfere with galectin-3 mediated cell adhesion.
- May reduce metastatic spread in experimental models.
- May influence immune activity and fibrosis.
- May complement—not replace—standard oncology care.
Human Evidence
Small clinical studies, particularly in prostate cancer, suggest possible slowing of PSA doubling time in some patients. However, large randomized trials demonstrating improved survival or prevention of metastasis are lacking.
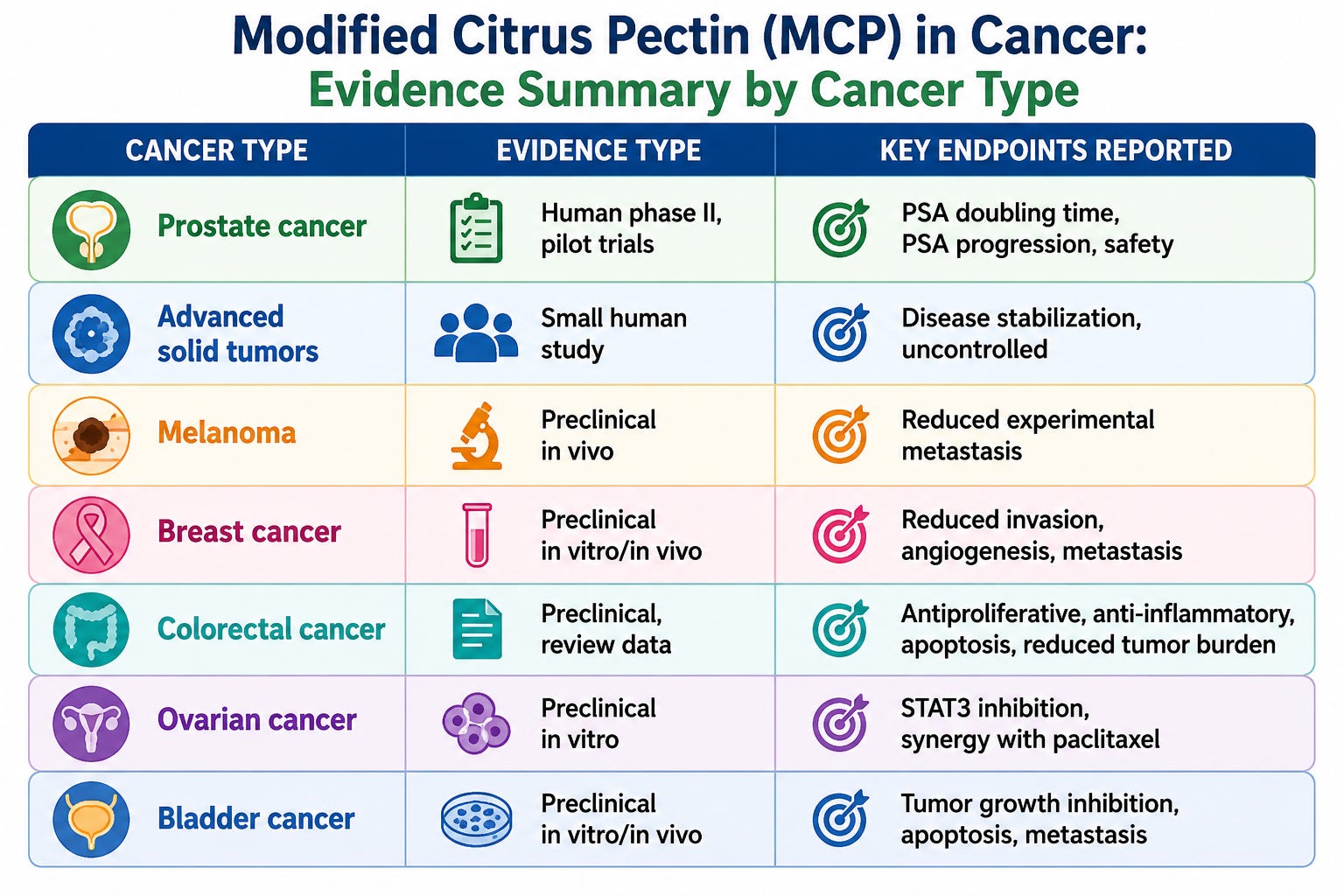
Modified citrus pectin (MCP) has the most human data in prostate cancer (biochemically relapsed, non‑metastatic), with additional preclinical data across several other tumor types including melanoma, breast cancer, colon cancer, ovarian cancer, bladder cancer, multiple myeloma, and hemangiosarcoma. (2)
Prostate cancer
A prospective phase II study of P‑MCP in 60 men with non‑metastatic biochemical relapse (rising PSA after local therapy) used 4.8 g three times daily for 6 months; 58 completed at least one month.(6)
MCP treatment was associated with lengthening of PSA‑doubling time in a significant subset and lower‑than‑expected rates of progression versus historical controls, with minimal toxicity, leading authors to conclude MCP “has a potential benefit and is safe” in this setting and warrants further trials.
Prior smaller pilot studies also suggested PSA‑DT prolongation in men with biochemical recurrence, which prompted a phase III trial (NCT01681823) evaluating MCP effects on PSA kinetics; full phase III outcome data are still limited/unclear in the public domain.
Advanced solid tumors
A 49‑patient pilot study in advanced solid tumors treated with modified (hydrolyzed) citrus pectin reported good tolerability, disease stabilization in a subset, and occasional minor responses, but no randomized control; it was framed as exploratory for safety and “clinical benefit” rather than definitive efficacy.(7) The study was summarized as follows: “MCP seems to have positive impacts especially regarding clinical benefit and life quality for patients with far advanced solid tumors. The presented preliminary data encourages us to further investigate the role of MCP in cancer prevention and treatment.”
Overall, human oncology data remain early‑phase, with signals in biochemical recurrence prostate cancer and disease stabilization in mixed solid tumors, but no robust survival or hard endpoint data yet. ClinicalTrials.gov ID NCT01681823
Cancers with preclinical evidence
Most other “signals” are preclinical (in vitro and animal models), often via galectin‑3 inhibition (adhesion, apoptosis, angiogenesis, metastasis).(8)
Melanoma – Experimental metastasis models showed MCP reduced melanoma spread.(2)
Breast cancer – MCP inhibited invasion and metastasis of metastatic breast carcinoma cells, and reduced angiogenesis in mouse models.(2)
Colon/colorectal cancer – MCP and other modified pectins show antiproliferative and pro‑apoptotic effects in colorectal cancer models, with some data on reduced tumor burden in animals.(9)
Ovarian cancer – PectaSol‑C MCP inhibits galectin‑3–induced STAT3 activation and synergizes with paclitaxel in SKOV‑3 multicellular spheroid models.(10)
Bladder (urothelial) cancer – MCP reduced proliferation, induced cell‑cycle arrest and apoptosis, and significantly inhibited T24 xenograft growth in mice via galectin‑3–dependent mechanisms.(8)
Multiple myeloma – MCP reversed galectin‑3–mediated resistance to bortezomib and enhanced dexamethasone‑induced apoptosis in myeloma cells.(2)
Hemangiosarcoma and endothelial tumors – MCP reduced clonogenic survival, increased sensitivity to doxorubicin, and inhibited angiogenesis and spontaneous metastasis in mouse models.(2)
Safety and tolerability
Across oncology and cardiovascular trials, MCP has been generally well tolerated at doses around 4.8–15 g/day, with adverse events mostly limited to mild GI symptoms (bloating, loose stools, nausea).(7)
No significant hepatotoxicity, nephrotoxicity, or myelosuppression has been observed in published clinical trials, and phase II prostate data report “no significant toxicity,” but long‑term safety beyond 1–2 years is not well characterized.(11)
Regulatory and guideline status
MCP is marketed as a dietary supplement rather than an approved drug; there is no major oncology guideline (e.g. NCCN, ESMO) endorsement for its use as standard cancer therapy, and patient information resources like Cancer Research UK describe the evidence as “very early” and experimental.
ClinicalTrials.gov lists several completed and ongoing studies, mostly in prostate cancer and cardiometabolic contexts, underscoring its status as an investigational adjunct rather than a validated treatment.
Practical considerations (oncology context)
Typical research doses in prostate BRPC: 4.8 g TID of a defined MCP product (e.g., PectaSol‑C), taken away from food to improve absorption, for 6–12 months or until progression.
From a risk–benefit standpoint, in a patient interested in integrative approaches, MCP could be considered a low‑toxicity experimental adjunct in BRPC or advanced solid tumors, with counseling that evidence is limited, endpoints are largely surrogate (PSA, stabilization), and it should not replace effective standard therapies.
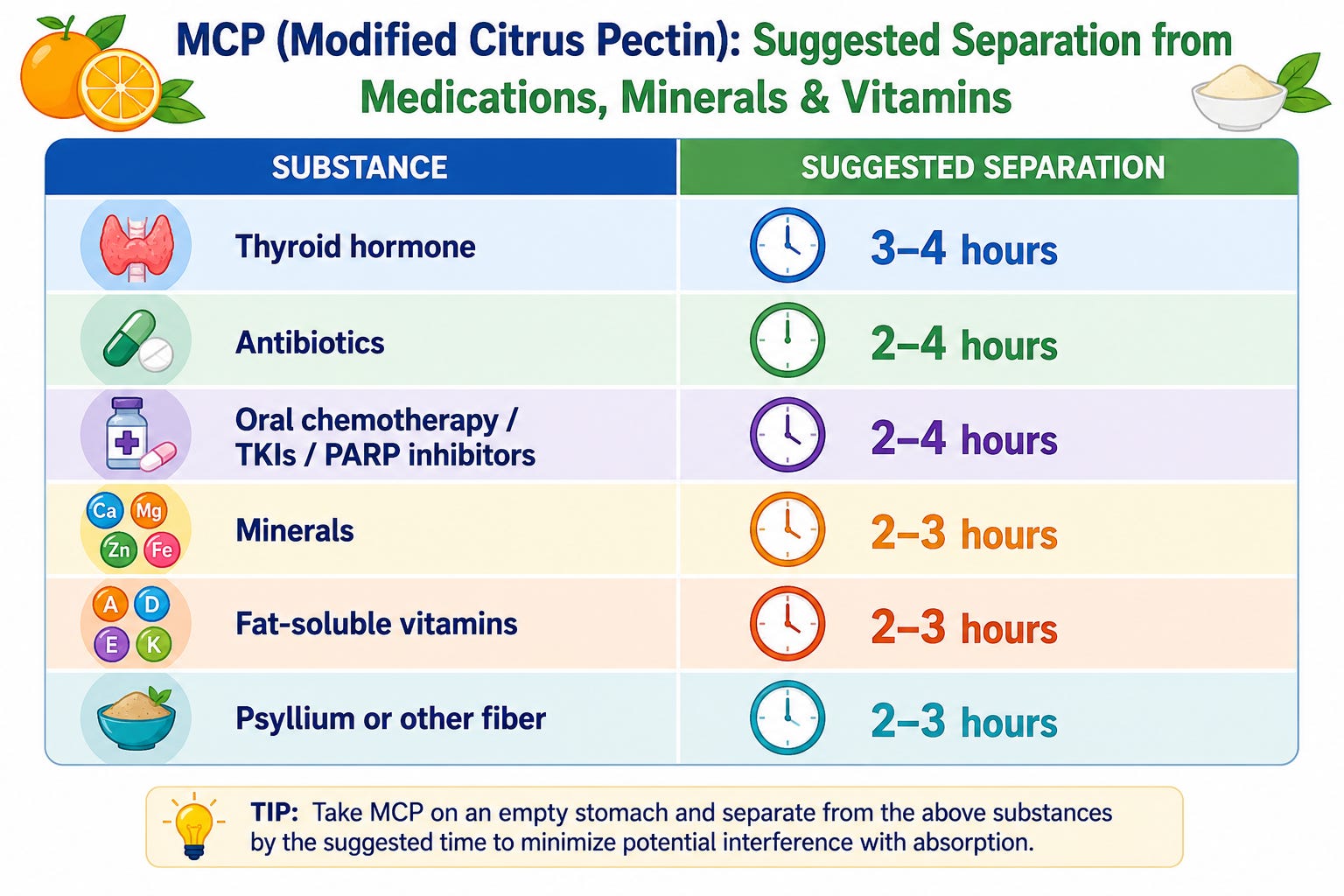
Timing of administration
This is very problematic as MCP interferes with the absorption of several drugs, minerals and nutraceuticals and food interferes with the absorption of MCP.
Modified citrus pectin (MCP) can interfere with the absorption of certain medications and nutrients, though the extent varies depending on timing and dosage. Pectin molecules contain negatively charged carbohydrate structures that can bind or complex with other compounds in the intestinal lumen. The concern is that MCP could bind drugs, minerals, or other supplements and reduce the free fraction available for absorption. Furthermore, soluble fibers can increase intestinal viscosity. Even modest gel-like behavior may slow movement of drugs toward the intestinal wall. This can delay or reduce absorption, especially for drugs that already have limited bioavailability. Reviews of plant fibers and bile-acid interactions describe viscosity and impaired micellar mobility as key mechanisms by which fibers influence intestinal absorption.
MCP can reduce absorption of several medications by 20-40%, particularly affecting:
minerals such as iron, zinc, magnesium, calcium
thyroid hormone
antibiotics, especially tetracycline antibiotics
oral chemotherapy or targeted drugs
digoxin (Lanoxin)
narrow-therapeutic-index drugs
statins
blood pressure medications such as ACE and ARB’s
Clinical implication
MCP behaves pharmacokinetically like a soluble fiber: its main interaction is binding and reducing absorption, not CYP-mediated metabolism effects.
Extra caution is warranted with narrow-therapeutic-index agents (e.g., digoxin) and critical antibiotics, where even modest reductions in exposure may matter clinically.
For polypharmacy, a simple rule is to treat MCP like a “gut binder”: schedule it away from morning and evening medication clusters by at least 1–2 hours when feasible.
Table 1. Suggested time separation between various medications and MCP
Practical Clinical Considerations
The fiber content of MCP is responsible for most absorption interference, as it can bind to substances in the digestive tract. To minimize interactions, separate MCP administration from other medications and supplements by 2-4 hours. Since repurposed drugs and nutraceutical combinations are the primary intervention for cancer patients, timing protocols become critically important when combining MCP with other repurposed drugs or supplements.
The best time to take MCP is 30 minutes before a meal or 2 hours after eating on an empty stomach, while maintaining at least a 2-hour buffer from all medications and mineral supplement. The best approach may be to anchor MCP in a consistent mid-morning or mid-afternoon slot to avoid medication “clusters” typically taken at breakfast and bedtime. Maintain consistent daily timing.
It is unfortunate that this critical information is not printed on the medication label nor the manufacturers website.
Table 2. Level of evidence summary by type of cancer
FAQ
Can MCP cure cancer?
There is currently no high-quality evidence showing MCP cures cancer.
Can it reduce metastasis?
Laboratory evidence suggests anti-metastatic potential, but definitive human evidence is still insufficient.
Medical Disclaimer
This article is for educational purposes only and is not medical advice.
- Dr Paul Marik - "Modified Citrus Pectin: The Anti-Metastatic Supplement Most Oncologists Ignore" (May 2026)
References
1. Leclere L, Cutsem PV, Michiels C. Anti-cancer activities of pH- or heat-modified pectin. Front Pharmacol. 2013;4:128.
2. Glinsky VV, Raz A. Modified citrus pectin anti-metastatic properties: one bullet, multiple targets. Carbohydr Res. 2009;344(14):1788–91.
3. García-Revilla J, Boza-Serrano A, Espinosa-Oliva AM, Soto MS, Deierborg T, Ruiz R, et al. Galectin-3, a rising star in modulating microglia activation under conditions of neurodegeneration. Cell Death Dis. 2022;13(7):628.
4. Ismail R, Habib HA, Anter AF, Amin A, Heeba GH. Modified citrus pectin ameliorates methotrexate-induced hepatic and pulmonary toxicity: role of Nrf2, galectin-3/TLR-4/NF-κB/TNF-α and TGF-β signaling pathways. Front Pharmacol. 2025;16:1528978.
5. Kassab AE. The Most recent updates on pectin in Cancer therapy: A review. Int J Biol Macromol. 2025;326:147331.
6. Keizman D, Frenkel M, Peer A, Kushnir I, Rosenbaum E, Sarid D, et al. Modified Citrus Pectin Treatment in Non-Metastatic Biochemically Relapsed Prostate Cancer: Results of a Prospective Phase II Study. Nutrients. 2021;13(12).
7. Azemar M, Hildenbrand B, Haering B, Heim ME, Unger C. Clinical Benefi t in Patients with Advanced Solid Tumors Treated with Modifi ed Citrus Pectin: A Prospective Pilot Study. Clinical Medicine Oncology. 2007;1:73–80.
8. Fang T, Liu DD, Ning HM, Dan L, Sun JY, Huang XJ, et al. Modified citrus pectin inhibited bladder tumor growth through downregulation of galectin-3. Acta Pharmacol Sin. 2018;39(12):1885–93.
9. Ornelas AC, Ferguson S, DePlaza M, Adekunle T, Basha R. Anti-Cancer Pectins and Their Role in Colorectal Cancer Treatment. Onco Ther. 2022;9(2):43–55.
10. Hossein G, Halvaei S, Heidarian Y, Dehghani-Ghobadi Z, Hassani M, Hosseini H, et al. Pectasol-C Modified Citrus Pectin targets Galectin-3-induced STAT3 activation and synergize paclitaxel cytotoxic effect on ovarian cancer spheroids. Cancer Med. 2019;8(9):4315–29.
11. Lau ES, Liu E, Paniagua SM, Sarma AA, Zampierollo G, López B, et al. Galectin-3 Inhibition With Modified Citrus Pectin in Hypertension. JACC Basic Transl Sci. 2021;6(1):12–21.

.png)




.png)



Comments
Post a Comment