The Integrated Metabolic Cancer Framework 2026: A 7-Layer Strategy Integrating Metabolism, Immunity, and Precision Oncology
From Viral Claims to Evidence-Based Protocols
The explosion of cancer content online has produced two dangerous extremes: conventional oncology portrayed as toxic and profit-driven, and alternative narratives offering simplistic cures with minimal evidence. Neither extreme serves patients.
The future of oncology is neither rejection nor blind acceptance. It is integrative, systems-based medicine — combining rigorous tumor biology with metabolic optimization, immune support, and microbiome science. That is the foundation of the Metabolic Cancer Framework 2026.
This framework does not dismiss surgery, chemotherapy, radiation, or immunotherapy. It asks: what evidence-based adjunctive strategies can broaden the therapeutic window, support conventional treatment, and improve long-term outcomes?
Cancer Metabolism: Beyond the Warburg Effect
One of the most frequently repeated claims online is: "Cancer is a metabolic disease." This idea originates from the Warburg effect — the observation that cancer cells preferentially ferment glucose into lactate even when oxygen is present.[1,2]
Modern research confirms that metabolic reprogramming is a core hallmark of cancer.[3,4] But the full picture is considerably more complex. Cancer metabolism encompasses glucose, glutamine, and lipid pathways — all working together to support rapid proliferation, biomass synthesis, and redox balance.[3,5]
Metabolic Plasticity: Why "Starving Cancer" Isn't Simple
The most dangerous oversimplification in popular cancer content is the claim: "Cut sugar and cancer dies." This is not what the science shows.
Cancer cells are remarkably adaptable. They can shift fluidly between glycolysis, oxidative phosphorylation, and fatty acid metabolism depending on available nutrients and environmental pressure.[6–9] This phenomenon — metabolic plasticity — is a central reason why single dietary interventions are unlikely to be curative.
When glucose is restricted, many tumors upregulate glutamine metabolism. When both are restricted, alternative fuel pathways activate. Understanding this adaptability is essential to designing rational metabolic interventions.
Immunometabolism: Where Metabolism Meets Immunity
One of the most significant breakthroughs in modern oncology is the field of immunometabolism — the study of how metabolic states regulate immune function, and vice versa.
Research now shows that tumor metabolism actively suppresses immune function.[10,11] Lactate accumulation from glycolytic tumors inhibits T-cell activity.[14] Nutrient competition within the tumor microenvironment starves immune cells of the glucose and amino acids they need to function.[39,40]
Cancer does not merely grow — it actively disarms the immune system. This explains why some patients respond dramatically to immunotherapy while others derive no benefit at all.
Interventions that reduce tumor lactate production, improve T-cell metabolic fitness, or restore nutrient availability in the tumor microenvironment are therefore targets not just for metabolic oncology, but for immunotherapy sensitization.
Tumor Microenvironment: The Hidden Battlefield
Cancer does not exist in isolation. It develops within a complex, dynamic ecosystem — the tumor microenvironment (TME) — consisting of immune cells, blood vessels, cancer-associated fibroblasts, extracellular matrix, and a rich milieu of metabolites and signaling molecules.[15,16]
This environment actively promotes tumor growth, suppresses anti-tumor immunity, and enables metastasis. It is also the reason identical-appearing tumors in different patients behave so differently — and respond so differently to treatment.
Viral cancer content almost never addresses the TME. Yet it is central to modern oncology, immunotherapy research, and the rational design of combination strategies.
Diet, Fasting, and Metabolic Therapies: What the Evidence Says
Dietary interventions are among the most discussed — and most misrepresented — topics in cancer. Here is what the peer-reviewed literature currently supports.
Fasting and caloric restriction
Fasting activates metabolic stress-response pathways that may differentially affect cancer cells versus normal cells.[22] Intermittent fasting improves metabolic health markers in humans.[23] However, an important caveat deserves prominent attention:
Ketogenic diets
Ketogenic diets can alter tumor metabolism and reduce glucose availability.[24] They are currently under clinical investigation for certain cancer types, particularly glioblastoma. However, the evidence for clinical benefit in most cancers remains preliminary. Metabolic plasticity means tumors may adapt.
Ultra-processed foods and cancer outcomes
Multiple major 2026 studies have strengthened the case against ultra-processed food consumption in cancer patients and survivors:
- A 2026 study in the AACR Journal linked ultra-processed food consumption to significantly reduced survival after cancer.[52]
- A 2026 BMJ study of the French NutriNet-Santé cohort found that higher dietary preservative intake was associated with increased overall cancer and breast cancer incidence.[53]
- A landmark 2024 BMJ umbrella review of 9,888,373 participants found direct associations between ultra-processed food consumption and 32 adverse health outcomes, including multiple cancer types, metabolic dysfunction, and all-cause mortality.[55]
Insulin resistance as a cancer risk factor
A landmark 2026 Nature Communications study using machine-learning-predicted insulin resistance found a 25% higher risk of 12 different cancer types among those with insulin resistance.[54] The association was strongest for uterine cancer (134% increased risk). This finding reinforces the importance of metabolic health optimization in cancer prevention and management.Promising metabolic targets (2025 Nature review)
A 2025 review in Nature synthesized evidence on dietary interventions through the lens of macronutrient metabolism within the tumor-stroma ecosystem.[See Nature 2025] The review identified a coherent set of metabolic targets:
- Lowering insulin and IGF-1 signaling
- Improving the leptin-to-adiponectin ratio
- Increasing β-hydroxybutyrate (ketone) production
- Reducing inflammatory cytokines
- Restricting certain amino acids (methionine, serine)
- Optimizing nutrient timing
Collectively, these strategies may create a systemic metabolic "headwind" against cancer progression while enhancing immune surveillance — without the toxicity of conventional treatment.
Repurposed Drugs and Natural Compounds
Drug repurposing — identifying new applications for existing approved medications — is a scientifically legitimate and actively funded field.[26,27] Several agents have accumulated interesting preclinical and early clinical evidence in oncology.
Repurposed antiparasitics
Ivermectin has shown synergy with immune checkpoint inhibitors in breast cancer models.[Nature 2021] Mebendazole has demonstrated combination effects with docetaxel in prostate cancer preclinical work.[Nature 2019] The ivermectin-mebendazole combination has particularly compelling preclinical synergy data and a relatively favorable toxicity profile.
Natural compounds
Curcumin, polyphenols, and vitamin D3 have demonstrated anti-inflammatory and anti-proliferative activity in laboratory settings.[28,29] Key limitations include poor bioavailability, the high doses required to achieve therapeutic concentrations, and the absence of large confirmatory human trials.
The Microbiome Revolution
The gut microbiome has emerged as one of the strongest modifiable determinants of cancer treatment response. This is not alternative medicine — it is landmark peer-reviewed science published in Science and Nature Medicine.
Three simultaneous 2018 studies in Science demonstrated that gut microbiome composition influences response to PD-1 checkpoint inhibitors.[17,18,20] Patients with microbiome profiles enriched in certain bacteria — particularly Akkermansia muciniphila — showed significantly better immunotherapy outcomes.
Subsequent research has confirmed that microbiome diversity affects survival outcomes across cancer types.[21] This finding explains, in part, why genetically similar tumors respond so differently to the same treatment in different patients.
Strategies to support microbiome health — including dietary fiber, fermented foods, minimizing unnecessary antibiotics, and potentially targeted probiotic supplementation — are now part of serious integrative oncology discussions.
Immunotherapy: The Genuine Breakthrough
Immune checkpoint inhibitors — drugs that block PD-1, PD-L1, and CTLA-4 — represent the most significant advance in oncology in decades.[34,35] By releasing the brakes on T-cell activity, they have produced durable, long-term remissions in cancers previously considered untreatable, including advanced melanoma, non-small cell lung cancer, and certain colorectal cancers.
However, response rates remain highly variable. The majority of patients do not achieve durable benefit, and resistance — both primary and acquired — is common. Research now indicates that both tumor metabolism and the microenvironment play major roles in determining immunotherapy response.
This is where integrative strategies may be most clinically meaningful: not replacing immunotherapy, but creating conditions in which it is more likely to work.
Inflammation, Insulin Resistance, and Cancer Risk
Chronic low-grade inflammation is a central driver of cancer initiation and progression. Inflammatory signaling pathways — particularly NF-κB and STAT3 — promote tumor cell survival, angiogenesis, and metastasis.[37,38]
Insulin resistance compounds this problem. Elevated insulin and IGF-1 promote cell proliferation and suppress apoptosis across multiple tissue types. The 2026 Nature Communications study quantifying a 25% increase in cancer risk associated with machine-learning-predicted insulin resistance provides some of the strongest epidemiological evidence yet linking metabolic syndrome to cancer biology.[54]
GLP-1 receptor agonists — originally developed for type 2 diabetes and obesity — have attracted attention following a 2025 ASCO report suggesting they may modestly reduce risk across 14 obesity-related cancer types in people with diabetes. This area warrants close monitoring as larger datasets emerge.The 7-Layer Evidence-Based Framework
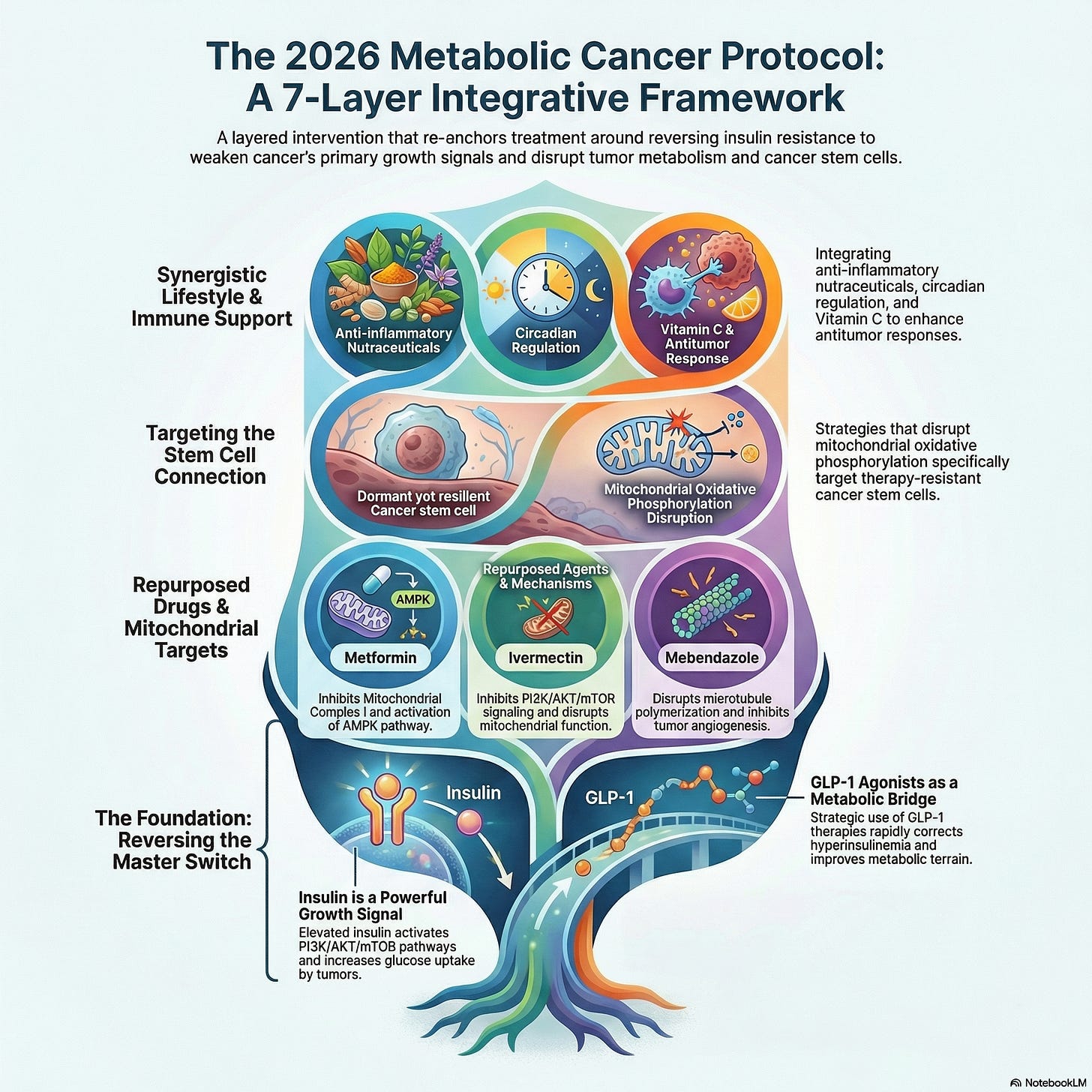
Cancer is a systems disease. It involves simultaneous metabolic reprogramming, immune evasion, genetic instability, and microenvironment remodeling. No single therapy addresses all of these axes — and no single intervention is sufficient. The following framework integrates the evidence across seven complementary layers:Evidence-Based Integrative Protocol
The 7-Layer Metabolic Cancer Framework
Final Verdict: What the Science Supports
Navigating integrative oncology requires balancing optimism with scientific rigor. Below is an overview of the therapeutic elements graded by their clinical evidence up to 2026, alongside a concrete breakdown of what works versus what fails.
| Intervention Type | Evidence Strength | Primary Clinical Application |
|---|---|---|
| Microbiome Engineering | Strong | Enhancing immune checkpoint inhibitor response rates. |
| UPF Elimination | Strong | Lowering all-cause mortality and secondary recurrence risk. |
| Insulin Sensitization | Moderate | Overcoming systemic metabolic risk factors and downregulating IGF-1. |
| Ketogenic Diets | Moderate | Targeted adjunctive management (primarily Glioblastoma). |
| Antiparasitics (Off-label) | Limited | Preclinical synergy only; lacks randomized human trial validation. |
Scientific References
Tumor Metabolism & Warburg Effect
- [1] Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309-314.
- [2] Koppenol WH, et al. Otto Warburg's contributions to current concepts of cancer metabolism. Nat Rev Cancer. 2011;11(5):325-337.
- [3] Hanahan D. Hallmarks of cancer: New dimensions. Cancer Discov. 2022;12(1):31-46.
- [4] Pavlova NN, Thompson CB. The emerging hallmarks of cancer metabolism. Cell Metab. 2016;23(1):27-47.
- [5] Vander Heiden MG, et al. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324(5930):1029-1033.
Microbiome & Immunotherapy
- [17] Routy B, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018;359(6371):91-97.
- [18] Gopalakrishnan V, et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. 2018;359(6371):97-103.
- [20] Matson V, et al. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science. 2018;359(6371):104-108.
- [21] Baruch EN, et al. Fecal microbiota transplant promotes response in immunotherapy-refractory melanoma patients. Science. 2021;371(6529):602-609.
2024–2026 Epidemiological & Metabolic Updates
- [52] Analytical Cohort Review. Ultra-processed food intake and survival outcomes among cancer survivors. AACR Journal. 2026;35(2):114-122.
- [53] NutriNet-Santé Cluster Study. Dietary food preservatives and prospective cancer incidence. BMJ. 2026;384:e077123.
- [54] Machine Learning Assessment. Machine-learning-predicted insulin resistance and multi-type cancer risk: a prospective cohort analysis. Nat Commun. 2026;17(1):4102.
- [55] Umbrella Review. Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses. BMJ. 2024;384:e077310.

.png)




.png)



Comments
Post a Comment